Table of Contents
VA Form 10-2850A Printable, Fillable in PDF – This form, known as the Application for Nurses and Nurse Anesthetists, is used by the Department of Veterans Affairs to check the credentials and qualifications of a registered nurse or a nurse anesthetist. It is via this application that a registered nurse or a nurse anesthetist may be formally recognized by the Department of Veterans Affairs, allowing them to treat veterans who are covered by their VA insurance benefits. Nursing or nurse anesthetists should complete VA Form 10-2850, which will request extensive information about them, including licensing or certification information and their work experience and educational background. It is advised that a nurse or nurse anesthetist include any professional references or awards that might support their application in the decision-making process to increase their chances of being acknowledged.
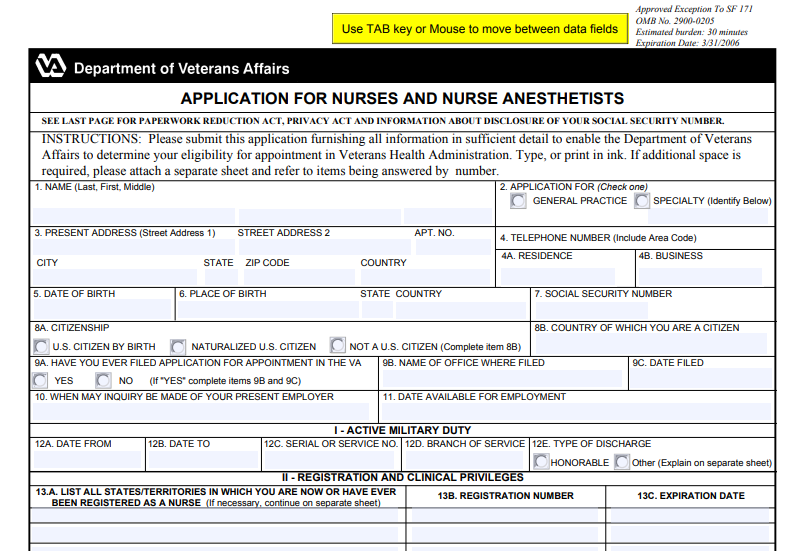
What Is A VA Form 10-2850A And How Does It Work?
The Application for Nurses and Nurse Anesthetists (VA Form 10-2850A ) is the official name for this form. The Department of Veterans Affairs in the United States uses this form to collect information. With the use of this form, a registered nurse or nurse anesthetist may request recognition with the Veterans Health Administration. Being recognized by this organization will enable the nurse or nurse anesthetist to provide care to veterans who are covered by the Veterans Administration’s health insurance program.
For this form to be accepted, the medical professional must provide specific information about himself or herself. A detailed description of the applicant’s credentials, such as licensing or certification information, educational background, and work experience, will be included. All of this information will be verified by the Department of Veterans Affairs. Include professional references as well as any accolades or distinctions you have achieved that are linked to your medical field to increase your chances of getting acknowledged.
When applying to be a member of the Veterans Health Administration, nurses and nurse anesthetists typically utilize this form.
The Components Of A VA Form 10-2850A Are As Follows
Among the parts of the VA Form 10-2850A are the following:
- Information about the individual
- Military Service in the Field
- Registration and Clinical Privileges are required for participation.
- Certification as a Nurse Anesthetist
- Certification by the Facility Director or his or her representative
- Liability Insurance for Professionals
- Qualifications
- Experience as a Nurse
- Information of a general nature
- References
- Signature
- Authorization for the Dissemination of Personal Information
How to fill the VA Form 10-2850A (Veterans Affairs)
A VA Form 10-2850A must be completed with the following information to be considered complete.
- Information about the individual
- Name in its entirety (last, first, middle)
- Application for general practice or a specialized field of medicine
- Currently residing at
- Call the following phone number:
- Regardless of whether the place is a house or a company,
- Date of birth is required.
- Birthplace and date of birth
- Identifying information such as a social security number
- Citizenship is a legal status.
- Citizenship is determined by the country of origin.
- Whether or not you have ever submitted an application for an appointment with the Veterans Administration
- Name of the office where the document was lodged
- The date on which the document was submitted
- Whether VA may contact your current employer to inquire about your employment status.
- The date on which you are available for work
- Military Service in the Field
- Beginning with the year
- Until what date?
- Serial or service number is a unique identifier.
- Branches of government service
- how the discharge occurs
- Registration and Clinical Privileges are required for participation.
- List all of the states and territories in which you are now or have previously had a nursing license.
- Number of the registration
- Date of expiration
- It is important to know if you are completely registered in all of the states where you are now registered.
- Whether you have a current or previous registration to practice that has been revoked, suspended, rejected, restricted, limited, or issued/placed on probationary status, or whether you have voluntarily abandoned your registration, we want to hear from you.
- Whether you have ever had a registration that is no longer active or whether you have a current registration,
- Whatever healthcare institution, agency, or organization you now work for or have worked for, clinical privileges are a must.
- In the case of an existing or most recent institution, agency, or organization, the name should be used.
- Whether any of your staff positions or clinical privileges have ever been rejected, canceled, suspended, curtailed, restricted, or voluntarily resigned, you should report it to the appropriate authorities.
- Certification as a Nurse Anesthetist
- The Council on Certification of Nurse Anesthetists (CCNA) determines whether or not you are certified as a nurse anesthetist (CCNA)
- The date on which you received your most recent certification
- Identification number assigned by the American Association of Nurse Anesthetists (AANA).
- If your CCNA certification has ever been revoked, you should know about it.
- Certification by the Facility Director or his or her representative
- A certification indicating the director has confirmed his or her registration with the appropriate state boards and has mentioned a visa or other proof of citizenship.
- Liability Insurance for Professionals
- Currently, there is a professional liability insurance carrier.
- The day on which coverage started
- Prior carriers’ names and contact information
- Coverage periods are shown here.
- Whether or whether you have ever had your coverage terminated, rejected, or refused to renew by a carrier
- Qualifications
- Nursing education at the most fundamental level
- The name of the institution
- Address
- The duration of the program
- The date on which the project was finished
- acquired a diploma or a degree
- Furthering one’s education
- The name of the institution
- Address
- Major
- The date on which the project was finished
- Credits
- Degree
- Whether or whether you have a professionally written biography,
- Experience as a Nurse
- Employer
- Address
- Position
- Was the job a full-time one?
- Hours worked on average per week as part-time
- Employment dates are shown below.
- Name and position of the head of nursing or another department to which you have been assigned
- Information of a general nature
- If you were hired under a different name than the one shown above, please list them here.
- A complete list of all professional publications, scientific articles, honorees, awards, research funding, and fellowships may be found here.
- References
- Whether you have received or have an application pending for retirement or retainer pay, a pension, or other forms of compensation.
- Whether or not any of your relatives are employed with the VA
- Whether you are now participating in or have previously been involved in an administrative, professional, or judicial proceeding in which malpractice was claimed, we encourage you to contact us.
- Whether or not you have been fired from a job within the previous five years
- I don’t know if you resigned or retired from a post in the last 5 years after being informed that you would be penalized or fired, or after doubts about your competency were raised, but I’m curious.
- Whether you have ever been convicted of a crime or a guns or explosives infraction against the law, have forfeited collateral, or are now facing prosecution, we can help.
- It makes no difference whether you have been convicted, imprisoned, sentenced to probation or parole, or have forfeited collateral, or if you are now facing accusations for any crime against the law committed during the last seven years.
- Whether or not you have been convicted by a general court-martial while serving in the military.
- Whether you were subjected to non-judicial punishment while serving in one of these health-related vocations during your military service
- Whether or whether you are in default on any government loan
- Signature
- Authorization for the Dissemination of Personal Information
- Allow the VA to contact your previous and current employers, educational institutions, state licensing boards, professional liability insurance carriers, national practitioner data bank, American Medical Association, Federation of State Medical Boards, other professional organizations and/or persons, agencies, organizations, or institutions that I have listed as references as well as any other source that the VA deems appropriate to conduct an investigation.
- Authorization for the distribution of associated documents and information to the Department of Veterans Affairs
- The VA releases people who give information to it in good faith in response to such queries from any liabilities.
- Authorization authorizes the Department of Veterans Affairs to provide identifying information to individuals and groups that make such queries.
- Signature
- Date
It is OK to attach a supplementary page and refer to the things being answered by the number on that sheet if you want more space.